Summary of "Addressing challenges to implementation of the contraceptive guarantee of the Affordable Care Act," Politi et al., Journal of the American Medical Association, Feb. 16, 2016.
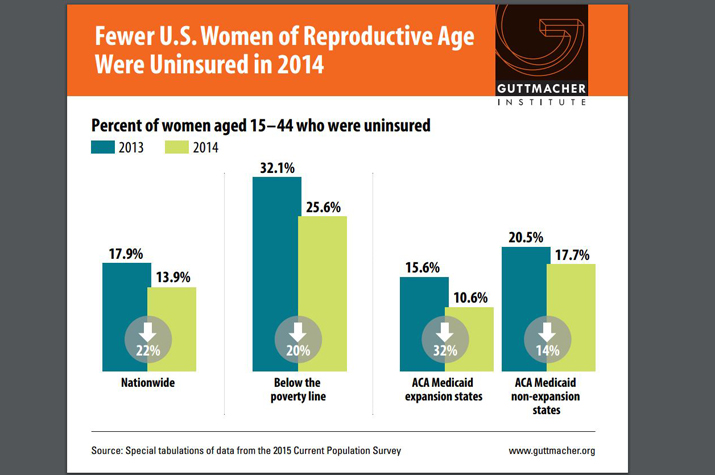
The Affordable Care Act's (ACA) contraceptive coverage rules have "directly benefited millions of women who use contraceptives by decreasing their total out-of-pocket spending on contraceptives," wrote Mary Politi of Washington University School of Medicine's Department of Surgery and colleagues. According to the researchers, the rules require private insurers to cover all FDA-approved "contraceptive methods, sterilization procedures, and patient education and counseling without any out-of-pocket costs."
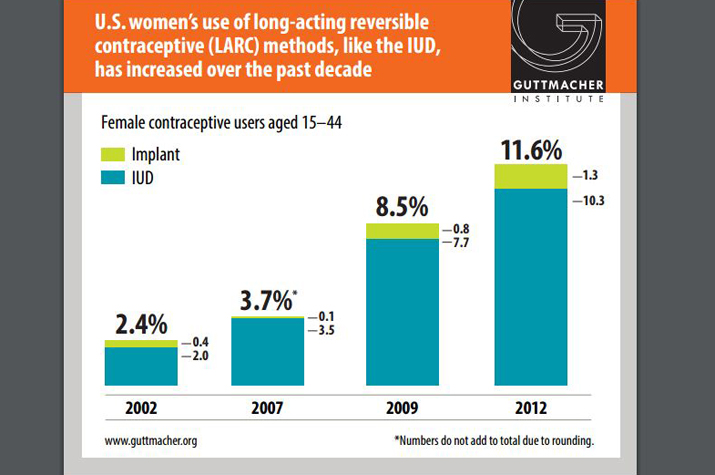
The researchers explain that prior to the law's implementation, financial constraints could have prevented women from using long-acting reversible contraceptives, which have "high initial costs," or from consistent use of "commonly used refillable methods, such as oral contraceptive pills, the contraceptive patch, or the vaginal ring with recurring prescription co-payments."
The researchers wrote that the contraceptive coverage guarantee has "the potential to substantially improve public health" by "reduc[ing] unintended pregnancies and births, which in turn can improve maternal and infant health" and enable women to "achieve their educational and workplace goals." Further, according to the researchers, insurers benefit under the law "because all methods [of contraception] are cost saving after accounting for the costs of unintended pregnancies and births."
However, the researchers noted that the provision's "guarantee is not absolute and does not apply to supplies (such as emergency contraception) obtained without a prescription nor does it apply to methods used by men." Moreover, health insurance "[p]lans can exclude coverage or require cost sharing for out-of-network services and supplies" and "[s]ome plans are exempt, including ... grandfathered plans (preexisting plans given a temporary reprieve from many ACA rules) and plans of some religious employers."
Implementation challenges
According to the researchers, "challenges to implementation exist for physicians and other clinicians, patients, and payers that may result in patients continuing to pay for all or part of covered contraceptive services."
Method choice
The researchers explained that some insurers offer only a limited selection of contraceptives without out-of-pocket costs. For example, some insurers "only cover generic versions of oral contraceptives or have excluded certain methods of contraception (eg, the vaginal ring) because they have a similar mechanism of action as oral contraceptives," the researchers wrote.
According to the researchers, "These issues should be ameliorated by the most recent federal guidance, released in May 2015, which states that plans 'must cover without cost sharing at least one form of contraception' in each of the 18 categories for women identified by the FDA."
Medical management
The researchers noted that the guidance permits insurers "to use 'reasonable medical management techniques' to control costs, but only within -- not across -- method categories." Further, according to the researchers, insurers are required under the guidance to "provide a clear and efficient process that 'is not unduly burdensome' to accommodate situations when a clinician recommends an uncovered method based on medical necessity." The researchers wrote that while insurers are obligated to "defer to the clinicians' recommendation" in such cases, "[i]t is not yet clear whether insurers have put such a process in place."
Noncontraceptive indications
According to the researchers, another barrier to implementation could result from confusion regarding contraceptives' off-label prescriptions, such as when "some women receive oral contraceptives or hormonal [intrauterine devices] to treat abnormal uterine bleeding."
The researchers wrote, "Although the federal guidance does not directly address such situations, these contraceptives still serve a contraceptive purpose and should therefore still be covered under the ACA's guarantee."
Clinical services
Under the ACA's contraceptive coverage rules, insurers must offer the "clinical services required to provide the contraceptive method ... with no cost sharing," such as "patient education and counseling, the injection or insertion of a contraceptive drug or device, anesthesia necessary for sterilization, follow-up care, and other related services," the researchers wrote."However, insurers have been inconsistent about covering such clinical services and federal guidance has not included every relevant example," the researchers explained, noting that such inconsistency could "lead to patients being erroneously charged for services that should be covered with no out-of-pocket costs, potentially interfering with patients' ability to practice contraception consistently and effectively."
Appropriate billing
Similarly, health care providers could face challenges with billing "for contraceptive services in a way that ensures that patients are properly exempt from cost sharing," the researchers wrote.
The researchers noted that while a woman who receives a prescription for contraception during a well-woman visit is covered under a specific billing code, there is no such code for a woman who visits a physician solely for the purpose of discussing contraception. As a result, providers must include a modifier when billing for such services. However, "[m]any clinicians and health organizations are unaware of this modifier, and some insurers have been slow to program their billing systems so that this modifier automatically triggers the patient's exemption from cost sharing," the researchers explained.
Diagnostic care
Additional problems can occur during visits that include diagnostic testing, "even when the initial visit was scheduled for contraceptive counseling or maintenance," because providers, insurers and even patients might be unaware of the preventive nature of such visits, the researchers wrote.
They explained, "Under the ACA provision, a visit should be considered preventive -- and therefore exempt from cost-sharing -- if the primary purpose of the visit is for preventive care." They wrote that while there are separate billing codes for preventive and diagnostic care, the dual options "could lead to confusion and disagreement about when patients will be charged." Improved transparency could help providers "communicate with patients about these potential fees," they wrote.
Out-of-network care
Another "complication is that insurers may exclude coverage or require cost sharing for out-of-network services and supplies, unless the service is unavailable in network," the researchers noted. They wrote that "patients and practitioners are not always aware of this limitation or the exception, and patients may not always realize that they are accessing out-of-network care." For example, the researchers explained that a woman undergoing a sterilization procedure at an in-network hospital might unintentionally be anesthetized by an out-of-network provider.
According to the researchers, this "out-of-network restriction also can apply to pharmacies."
Addressing the challenges
The researchers wrote that additional federal guidance on the ACA's contraceptive coverage rules "about such matters as the process for waiving medical management requirements or what qualifies as a preventive visit vs. diagnostic visit" would be helpful. "Beyond that, state regulators, insurance companies, and health care professionals each have their own responsibilities in addressing the challenges of implementing the contraceptive coverage guarantee," according to the researchers. Specifically, they noted that:
- State regulators must ensure that insurers "maintain health care networks that provide access to covered services" and could "prioritize network adequacy related to contraceptive care";
- Insurers should do more to comply with the ACA provision and be more transparent about coverage with patients and health care providers; and
- Health care professionals should better educate themselves and their patients, as well as improve their billing processes.
The researchers concluded, "Each of these steps could help ensure that the contraceptive coverage guarantee fully meets its potential to improve women's health and well-being."