In an article for The Nation, contributing writer Dani McClain writes about a new survey that found most experts in the delivery of long-acting reversible contraception are sensitive to the risk of coercive counseling in promoting LARC use.
According to McClain, the survey involved "104 researchers with clinical or social science expertise," 37% "of whom are clinicians who regularly provide implants or [intrauterine devices] to patients." McClain notes that 86% of the respondents were white, and as a result, the study did not draw conclusions "about how opinions differed by experts' race or ethnicity."
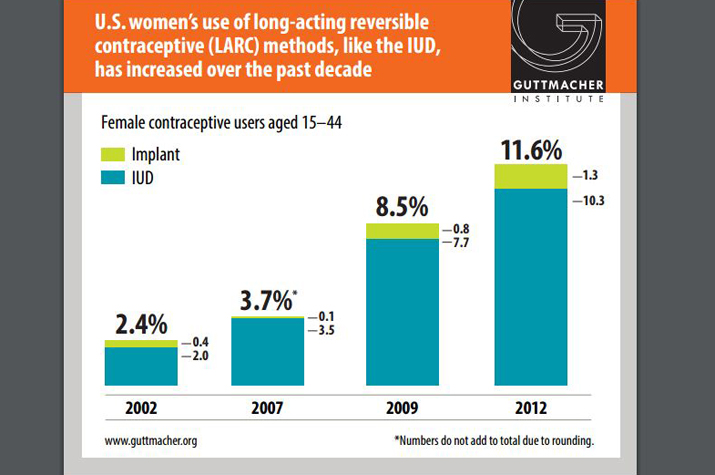
McClain writes, "Even if [LARC] devices were made more affordable and if education about LARC and training of providers improved, those surveyed largely anticipate that women in the United States would use [LARC] at rates similar to women in France or Norway, where between 25 percent and 29 percent of women use them." Further, respondents said "an uptake in LARC use alone cannot be counted on to reduce unintended pregnancy" and "other advances in contraception access should be pursued as well, such as providing over-the-counter access to the pill, dispensing one-year supplies of birth control, and developing new methods," McClain states.
McClain also touches on findings in the study related to coercive counseling. She explains that some reproductive-justice advocates are concerned "that health care providers, driven by conscious or unconscious bias, will disproportionately recommend the provider-controlled birth control method to women of color and [low-income] women."
According to McClain, the survey found that 98% of respondents "disagreed or strongly disagreed with this statement: 'Public assistance programs should be able to restrict benefits if a woman does not use a LARC method'"; 92% of respondents "disagreed or strongly disagreed with this statement: 'Corrections agencies should be able to offer reduced jail time if a woman uses a LARC method'"; and 91% of respondents "disagreed or disagreed strongly with this statement: 'Women receiving public assistance should have access to free LARC methods but not to less effective methods for free.'" Meanwhile, 97% of respondents "agreed that women receiving public assistance should have access to all forms of birth control for free."
McClain highlights a comment from one respondent, who wrote, "'We need a reproductive justice approach to LARC that starts with a woman's right to decide what's best for them and right to science-based, unbiased information about all contraceptive methods. We need to engage women of color who are leaders in reproductive justice work and community partners.'"
However, McClain writes that "respondents were split," largely along gender lines, "on whether to incentivize doctors and nurses to provide LARC to patients." According to McClain, "Two-thirds of men surveyed supported the idea of health plans and funding agencies setting higher LARC placement goals, compared to 30 percent of women surveyed." Meanwhile, "34 percent of men, but just 16 percent of women, supported the use of financial incentives for providers to place LARC." One respondent expressed concern that such incentives could influence providers to give care "that may not be in line with the patient's best interests."
McClain concludes that while the respondents to the study might be "more knowledgeable about these devices and not representative of the larger community of healthcare providers," the sensitivity they showed "to the possibility of coercion and their measured approach to setting expectations around more people choosing LARC is promising" (McClain, The Nation, 12/15).